


Midazolam Murder Mysteries: Who Is Dr Evans?
"A good death needs three things: equipment, medication and the staff to administer it." - Dr Evans


It is no secret that wall-to-wall mainstream media coverage of the so-called ‘lockdown files’ intends to turn guilty man Matt Hancock into fallguy, whilst simultaneously deflecting from the Midazolam Murders and trying desperately to insulate the UK government from the fallout.

Isabel Oakeshott — the slow-rolling supposed leaker — expresses disdain at the idea of Midazolam, insisting — without even checking — there’s no evidence, with the usual mainstream media pomp and circumstance of ‘conspiracy theory’.
Apparently the UK government have no idea how actual anti-lockdown advocates talk.

As other Twitter posters have noticed, Matt Hancock isn’t the sharpest knife in the drawer. Either you buy into the government stunt he handed a landslide of National Security violating evidence to a random female ‘journalist’, or you realise this is a hamfisted attempt at a cover up so bad and so rushed it looks like a child came up with it.
Either way, Matt Hancock isn’t ‘our guy’ — even if he does have blood on his hands — as these events are not just isolated to the UK. See Canada’s MAID, for example. Matt Hancock certainly didn’t tell Canada to kill the elderly. So, where do we go?
Well, one possible route is via the mysterious and not-talked-about Dr Evans, who unlike Matt Hancock, does have the qualifications to understand the ramifications of what they’re doing.
Before we get to the mysterious Dr Evans, we need to of course, form a proverbial chain of guilt.
Department Of Health And Social Care Is Guilty
Back in March 2020, the Department of Health and Social Care (DHSC) basically cleared out the entire Midazolam stock of a French pharmaceutical company — Accord Healthcare (Accord for short) — diverting resources from France.
Oddly, the DHSC boasted of this to The Pharmaceutical Journal:
Supplies of the sedative midazolam have been diverted from France as a “precaution” to mitigate potential shortages in the NHS caused by COVID-19, the Department of Health and Social Care (DHSC) has told The Pharmaceutical Journal.
They mentioned it included ‘four different strengths’, and in our findings, we found four different strengths had spiked in ordering:
The manufacturer said the French stock only includes midazolam at the strength of 1mg/mL in 5mL, while the initial supply in March 2020 contained a variety of four different strengths.
Accord have a rather catchy slogan:

Hmm, yes. Surely the now Midazolam dead elderly will appreciate that dark, indiscriminate irony.
Accord went on to note — showing you just how abnormal the Midazolam murders are — that the NHS cleared out two years worth of stock back in March 2020:
[…] it had to gain regulatory approval to sell French-labelled supplies of midazolam injection to the NHS, after having already sold two years’ worth of stock to UK wholesalers “at the request of the NHS” in March 2020.
The Pharmaceutical Journal then unintentionally point the finger at another organisation, the Royal College of Anaesthetists:
Midazolam is listed by the Royal College of Anaesthetists as a “first-line” sedative in the management of COVID-19 patients, and warns in guidance published on 2 April 2020 that it “may be subject to demand pressure”.
The Royal College of Anaesthetists
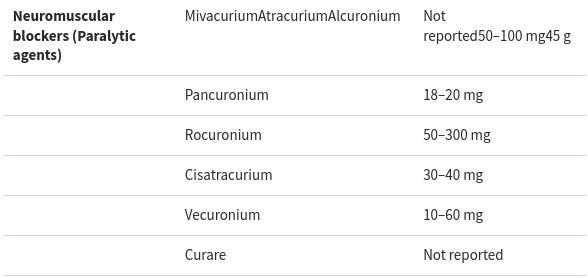
First line sedative? Seems abnormal. Their page (now archived) lists a number of End of Life drugs, and even a few assisted murder drugs, as ‘first line treatment’ for COVID-19.
For example, they list rocuronium, vecuronium and pancuronium:

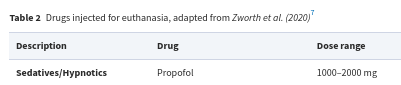
If you review the earlier assisted murder document we discussed in the Death Penalty Drugs Used By Care Homes article, you will find them listed, alongside more famous toxin curare.
In-fact, you will find many of the same drugs listed, such as Propofol:

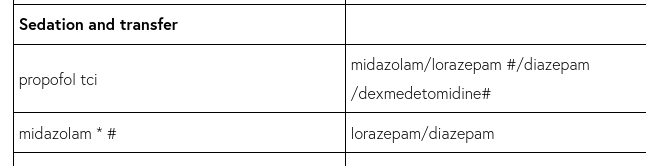
Or the usual suspects, Midazolam, Lorazepam, and also Diazepam:

And when was this ‘guidance’ issued? Same month as the spike in Midazolam prescriptions as before. 2nd April 2020 (one day before the NICE NG163 guidance):

Oh. So what drove this change?

For those of you not familiar with UK politics, Matt Hancock was the head of the Department of Health and Social Care, so if the DHSC ordered it, that was approved by Matt Hancock.
It might seem easy to blame Matt Hancock, after all, he is guilty, but Matt Hancock is not a doctor, however, so it is doubtful he’d know which chemicals save lives and which could kill. So who advised him to make the bulk orders?
Enter Dr Evans
In light of the evidence of the Midazolam murders in care homes, there is this frankly bizarre and disturbing exchange between a ‘Dr Evans’ and Matt Hancock, which take on a whole new meaning with the applied context.
Dr Evans asks Matt Hancock if Hancock has ordered enough ‘provisions’ for those he seems very confident will die at home:
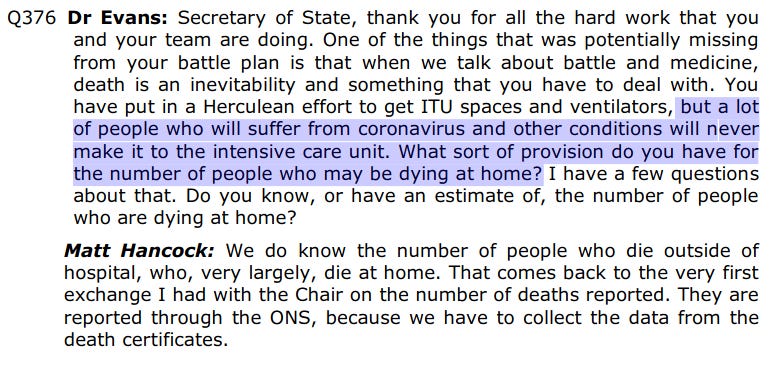
Matt Hancock replies he’s fully aware people will ‘die at home’. He seems very sure of himself for a non-doctor.
Dr Evans then advises Matt Hancock on how to ensure there’s a ‘good death’, and asks if Hancock has done the necessary bidding to ensure the NHS has enough ‘syringe drivers’ (the injection ampoules that we uncovered in The Death Penalty Drugs Used By Care Homes) :
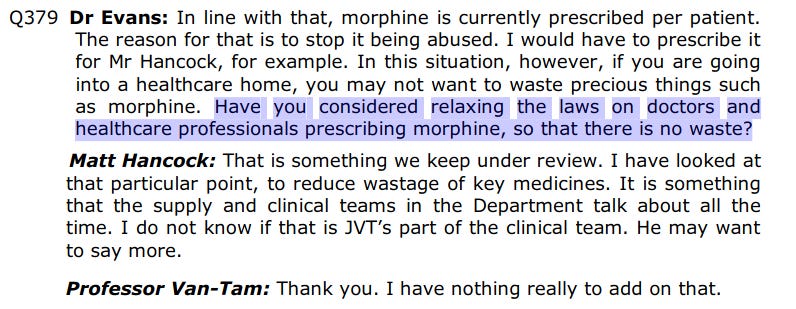
Despite Matt Hancock mewling how he’ll do the doctor’s bidding, Dr Evans seems very content to convict himself and say the quiet part out loud, and asks specifically about Midazolam and Morphine, the death-combo:

Matt Hancock replies ‘yes’, talking about how they have a “big project” to make sure “global supply chains” supply those drugs.
Dr Evans then suggests Matt Hancock relaxes the law on morphine without giving any valid reasons, likely so they can administer the drugs freely and on a whim:
There are no further directions from this ‘Dr Evans’, so who are they?
Dr Luke Evans
We can demonstrate this because he forms part of Matt Hancock’s ‘COVID inquiry’.

Dr Luke Evans is an MP, who completed their medical degree with the University of Birmingham in 2007, having been a “GP across the Midlands”. He talks about ‘clearing out the backlog caused by Covid’, which in this context is very dark, and boasts about being an elected member of the ‘Health and Social Care Committee’:

The description of the ‘Health and Social Care Committee’? Emphasis added:
The Health and Social Care Select Committee is a Departmental Select Committee of the British House of Commons, the lower house of the United Kingdom Parliament. Its remit is to examine the policy, administration and expenditure of the Department of Health and Social Care and its associated agencies and public bodies.
I.E. give advice to the Department of Health and Social Care.
Even as we speak, the so-called ‘Health and Social Care Committee’ is trying to retroactively justify mass murder by making an “inquiry” into assisted murder (read: invent a Parliamentary justification legalising the unethical and immoral behaviour they were caught engaging in):
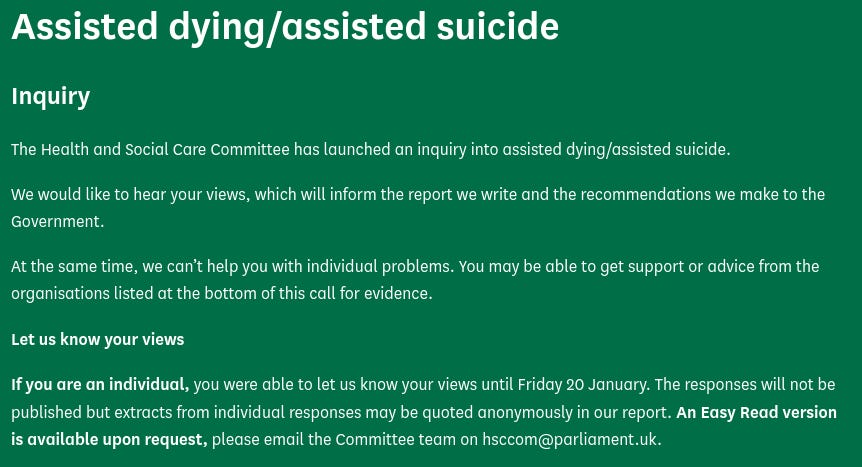

How surprisingly recent! Surely it has nothing to do with the fact the public are becoming aware the UK government murdered the elderly by stealth, so the government are trying to retroactively exonerate themselves from the crimes at Warp Speed?

Look beyond the fallguy, dear friends, and into the pit of oblivion that is the ‘Health and Social Care Committee’, which no doubt takes far more international influence than it first admits. After all, didn’t Rishi Sunak recently meet with the likes of Bill Gates? Who can forget Gates’ TedX talk about reducing the population?
American and Canadian sleuths, now is the time to investigate your own care homes for similar levels of wrongdoing. Just be aware, they may not have used the same set of drugs or the same dosages.
It is highly likely the UK weren’t the only ones doing this mass murder campaign, after all, so many countries moved in lockstep on the COVID-19 policies, why not also ones culling the elderly?
Subscribe to receive more content from The Daily Beagle.
Be sure to share these important stories!
And leave a comment below:
Sweden did the same. In Sweden, Dr Jon Tallinger, a GP, blew the whistle on euthanasia; he now works in Denmark instead of Sweden; "Instead of being given oxygen treatments at home or admitted to a hospital even when there is ICU capacity to treat them, the elderly and people over 60 with risk factors, Dr. Tallinger says, are often being prescribed morphine or other palliative pain medication (which does nothing to improve breathing) while being kept at home where they are essentially left to expire.
"How would you feel if you find out that your parent in the nursing home will not be given critical care, or curative care, or oxygen therapy, because they are deemed 'irrelevant,'" he wrote in a May 21, 2020 online essay.
"If an elderly patient eventually loses the fight with COVID-19, I say as a doctor that it is far more humane to let them die of narcosis and carbon dioxide after we have done our best to save the patient, instead of resorting primarily to morphine and breathing complications when they have contracted COVID-19 — all while denying them oxygen therapy and necessary medical attention," he wrote."
https://www.miamiarch.org/CatholicDiocese.php?op=Article_swedish-doctor-fights-for-elderly-victims-of-covid-19
Excellent series, UD! I'm going long on rope manufacturers.
Ativan and Xanax are the big benzos in the US. Ativan is very common in the hospital for its rapid onset. I'll have to dig around and see if one can even track prescriptions in the US much less from a nursing home or assisted living. Sales may be the only way. It's amazing to what one can have access. One glance at the FBI's yearly crime reports or the temperature data from GISS and know the Establishment is lying but health information can surprisingly difficult to access. Challenge accepted, dear writer!