


The Death Penalty Drugs Used By Care Homes
The Daily Beagle's Deep Dive Into Deadly Drugs


Credit to Alderamin, SuperCellex for doing valuable digging alongside, David Lamb for their story, and Denise Gardiner for their in-depth medical commentary. Thanks to Alan Richards for the BMJ update.
The Daily Beagle has spent the last several days digging through prescription datasets, BNF codes, documentation, forms, procedures, dosage limits, MHRA authorisations and more, and we come bearing blood-soaked receipts that it was indeed a Mass Murder of the Elderly.
This is probably one of the most explosive stories The Daily Beagle will cover.
Midazolam Is Literally Used For Lethal Injection

States can still use the sedative drug midazolam in lethal injections, according to today's Supreme Court decision. But how exactly does the drug work, and why do some say that it's unreliable?
— Live Science, “How Does Execution Drug Midazolam Work?”
This by itself would be damning. But this is just the beginning.
Midazolam Dosage Exceeds That Used In Death Penalty
In Arizona, the dosage for execution using midazolam is 50mg.
The Arizona execution protocol explicitly states that a prisoner will be executed using 50mg of hydromorphone and 50mg of midazolam
Do you know how much they give in UK palliative care homes? Here’s one care home’s listed advice from 2012:
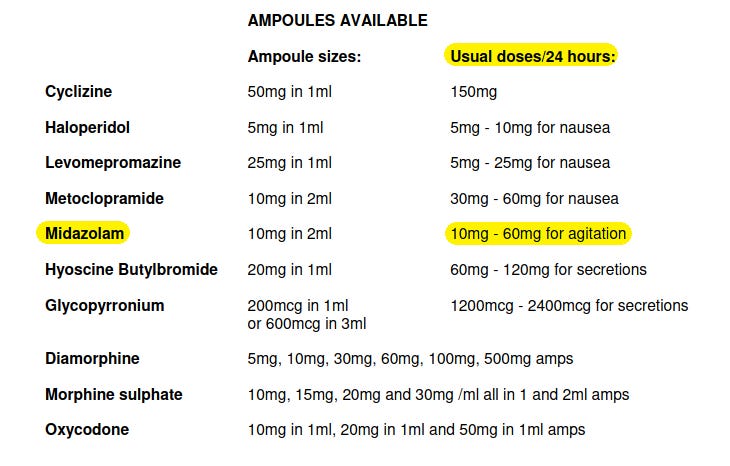
60mg in 24 hours. 10mg more than Arizona’s lethal injection!
Do you know how much Midazolam the MHRA recommends for someone over 60 years of age or with chronic illness?
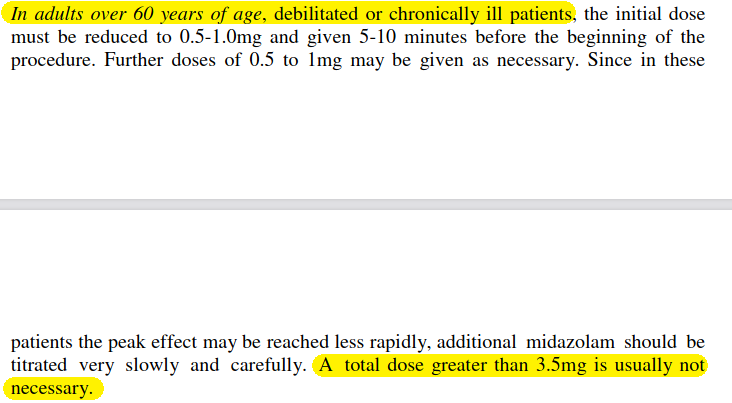
A mere 3.5mg. Total.
For a healthy adult below the age of 60, the MHRA advises this maximum total for Midazolam:

No greater than 5mg. And what do the End of Life care homes immediately start with? 10mg minimum.
Here’s another NHS End of Life UK website suggesting 20mg to 30mg Midazolam continuous infusion:

Reminder: NICE Issued Midazolam Guidance In April 2020
Although this was mentioned in the Mass Murdering Of The Elderly article, it’s worth re-mentioning the context here as it is very important.
On 3rd April 2020 — NICE (National Institute for Health and Care Excellence) issued guidance NG163 (NG — NICE Guidance) — which recommended the use of benzodiazepines, including Midazolam, for mere “agitation or distress”, directed at care homes:

NICE have since withdrawn that guidance, many months after, without explanation as to what prompted it. They issued the guidance despite admitting that drugs like Midazolam was not authorised for such purposes:

Numerous issues with the advice was raised by numerous medical specialists on the BMJ back in May 2020:
NG163 states: “Sedation and opioid use should not be withheld because of a fear of causing respiratory depression.” If COVID-19 infection were uniformly fatal, this would be an acceptable statement. But for people not previously known to be at the end of life, there is potential risk of unintended serious harm, if these medications are used incorrectly and without the benefit of specialist palliative care advice.
Another concern is that the recommended doses for morphine and midazolam are sometimes higher than current guidelines state for non-specialist use; and moreover there are inconsistencies between the maximum doses recommended by the oral or subcutaneous routes.
Orders For 10mg Midazolam Spike In April 2020
The Daily Beagle did a breakdown on the Midazolam ordering spike to get specific dosage orders. Remember, MHRA advise no more than 3.5mg total for the over 60s:
Notice how the strongest dosage for Midazolam (10mg diluted in just 2ml) is the one with the biggest jump, to ~7k orders?

Note, these are just the quantities the deliveries are made in. There’s nothing stopping staff members from administering multiple doses. But the minimum is 10mg. They can order smaller, more dilute doses (2mg, 5mg, etc), but they mostly don’t.
And we know they were dying in April 2020, per the peer-reviewed paper Antipsychotic prescribing to people with dementia during COVID-19:

“The number of deaths was nearly three times more than expected”.
Was it due to a lack of COVID-19 known treatment options? No! Hydrochloroquine prescriptions rose in March 2020, and Hydrochloroquine trials started on 3rd April 2020, the same day NICE issued guidance.

Midazolam Is A Terrible Way To Die
Midazolam is not a pleasant drug to be killed with either. A sedative with no painkilling properties. It makes you sleep but you still feel everything.
Midazolam is especially problematic because it’s not an anesthetic. As one of its inventors testified, midazolam induces drowsiness or sleep but it doesn’t stop a patient from feeling pain. Multiple people executed in recent years using midazolam have shown signs of pain—gasping, heaving against restraints, choking, and coughing.
— Equal Justice Initiative, “Lethal Injections Cause Suffocation and Severe Pain, Autopsies Show”
Do you know how care homes hide this ‘choking’, and ‘coughing’? It’s called the ‘death rattle’, where pages peddle unevidenced claims the dying person isn’t feeling any discomfort whilst having these breathing difficulties.

If it doesn’t cause discomfort, why do they seek to hide the struggle from onlookers?
Hiding The Struggle
In order to avoid disturbing the people watching, they use a class of drugs known as ‘anticholinergics’, that also have ‘antisecretory’ effects.
Anticholinergics are substances that block the action of the neurotransmitter called ‘acetylcholine’, interfering with the parasympathetic nervous system (AKA a ‘muscarinic receptor blocker’), and thus interferes with the muscles. They also reduce the production of such things like saliva.
It just so happens anticholinergics are also used with dementia and Alzheimer’s patients:
They are typically used to manage symptoms of Alzheimer’s disease and dementia.
Such drugs include (but are not limited to): Hyoscine Butylbromide, Buscopan (brand name), Hyoscine Hydrobromide and Glycopyrronium Bromide. Hyoscine is also known by the name Scopolamine.
Scopolamine (Hyoscine) Causes Amnesia
It is “horrible stuff”, says Curran. “When I used to give it to people [in experiments], they hated it – it makes your mouth really dry, it makes your pupils constrict. Certainly high doses would be completely incapacitating.”
Scopolamine has marked amnesic effects, and is used in Alzheimer’s research.
Anticholinergics Spike
The Daily Beagle found evidence of spikes in April 2020 for all of the above:
Hyoscine butylbromide 20mg/1ml inj ampoules (highest at 5k)






Following Assisted Murder Trail Uncovers More Spikes
Anticholinergics are also heavily used in the assisted murder field, especially during the final stages of death.
Maybe, desperate fellows might argue the administration of Midazolam — in blatantly fatal doses — is mere coincidence, and ‘there’s a reasonable explanation if you just give me a chance officer’.
Alas, not so. The Daily Beagle obtained a list of drugs used in assisted murder. Peer-reviewed, of course. Nothing but the best for our readers (highlighting added).
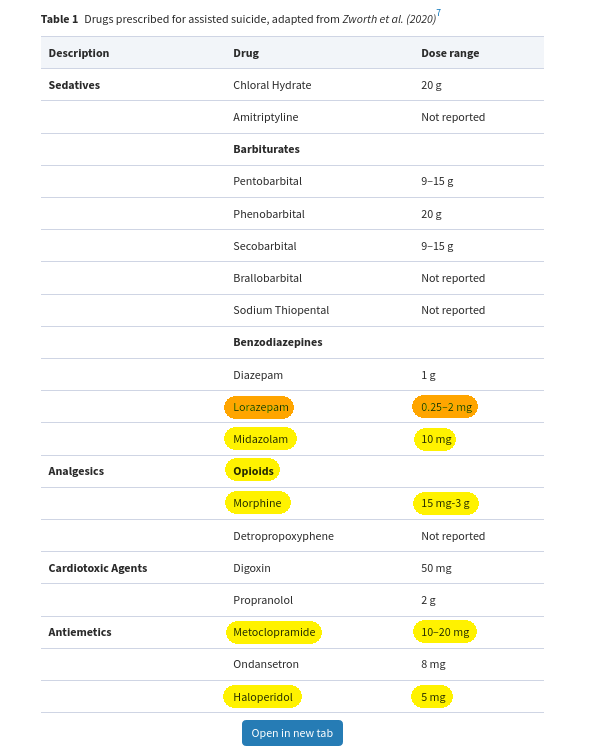
Highlighted in yellow are all the drugs that spiked in April 2020, along with their lethal dosages as used in assisted murder.
Notice the minimum amount for Midazolam on this list is a mere 10mg — the minimum dosage care homes are giving patients. We’ll get to the other drugs shortly.
Lorazepam
Highlighted in orange is Lorazepam that is prescribed so frequently — into tens of thousands range — that frankly no spike is even necessary. It is for the 1mg tablets.
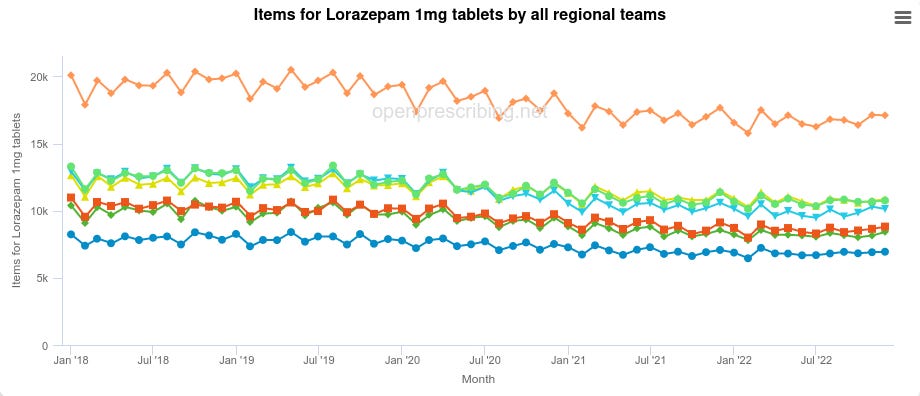

Notice the minimum dosage required for Lorazepam in assisted murder — 0.25mg — is so low, that even a tablet with poor bioavailability (read: bad uptake) would meet this criterion. Normally IV (intravenous; read: injectables) give 100% bioavailability, but with such low requirements IV isn’t even needed here. Note other drugs are injectables, except where otherwise noted.
Oh, and Lorazepam is also used by Canada’s MAID:

The same medical assisted murder that has killed over 30k in Canada.
In 2018, of the MAiD cases in Canada with available data, 50% were unsuccessful by 60 min and the clinician transitioned to euthanasia to complete the ‘assisted’ death.
— British Medical Bulletin, Efficacy and safety of drugs used for ‘assisted dying’
Morphine (Opioids)
Morphine spikes across five separate ordering domains (sulphate is the British spelling, sulfate the American; oddly, the NHS prescribing site uses the American spelling sulfate):
Even with all domains combined, the spike only goes up to 300…

Morphine is however an opioid, and there are plenty of alternative opioids. One such alternative is diamorphine, which saw weak spikes in April 2020:
Another alternative opioid — listed on palliative care — is Oxycodone, which enters the thousand range in April 2020:

Combining the various opioids together we see ~3k in April 2020:
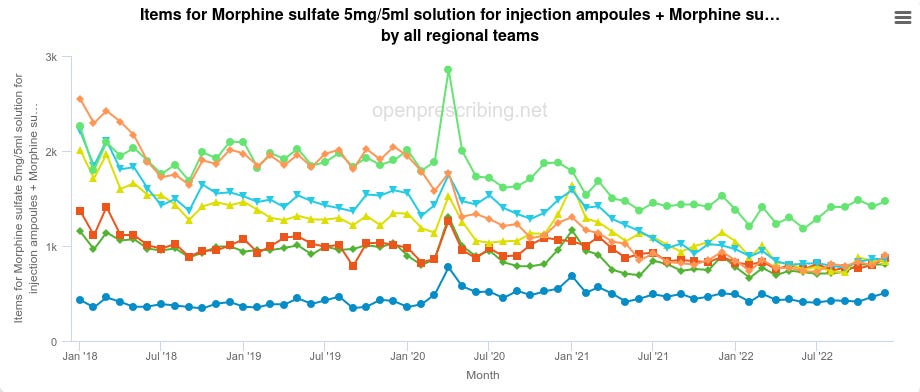

Whilst these order dosages aren’t quite the 15mg lethal dosage for assisted murder, 10mg injectable form is very close, and these are only the ordering quantities, not the administration quantities. There’s nothing stopping repeat dosages.
Another website gives a different lethal dosage — still easily achieveable:
A lethal dose of morphine may be as low as 120 mg for morphine tablets and 25 mg for intravenous solutions.
Remember, these are the injectable form of the drug. So the 15 to 25mg intravenous range applies here.
Haloperidol
Lethal dosage on the assisted murder document is 5mg:

The 5mg dosages are what spike in April 2020:

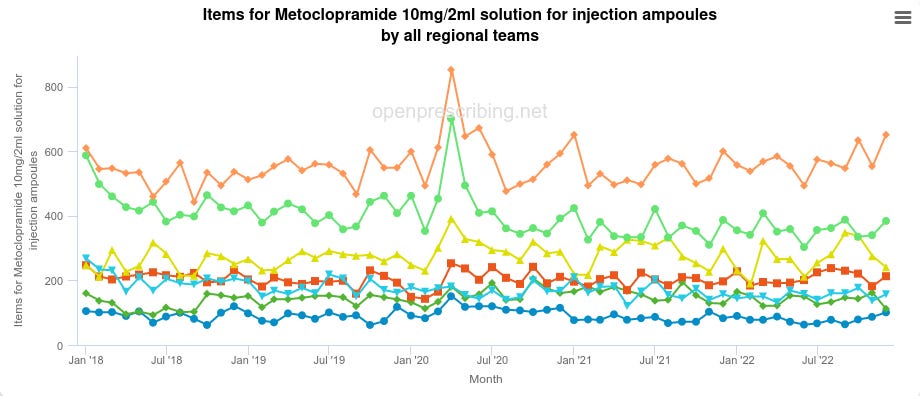
Metoclopramide
The lethal dosage required for assisted murder is 10 to 20mg:

Surprise, the 10mg dosages spike April 2020:
These Drugs Are Used In End Of Life ‘Care’
These weren’t the only drugs that spiked, either. Following the view it is State-sponsored mass murder, we looked at drugs used in UK’s End of Life ‘care’.
For example, this end of life document mentions many of the drugs we have shown that spike:

On this list are two we haven’t covered yet: Cyclizine, and Levomepromazine.
Cyclizine
Corresponding with the ampoule sizes on the above document, Cyclizine spikes in April 2020:

As we see from the end of life document, the elderly are given 150mg in the space of 24 hours (remember, intravenously, so 100% bioavailability):

NHS Scotland echoes similarly, calling for, up to 150mg in 24 hours. They even admit the “subcutaneous infusion” (subcutaneous means ‘below skin’, infusion is usually an IV drip feed or similarly; read: injection) is an “unlicensed route”, I.E. unapproved (but notice not stopped by the government):

According to PubChem, the ‘probable’ toxicity of Cyclizine for a human is 5 to 50mg per kg:

PubMed reports a toxicity range starting at 5mg per kg, and climbing up to 80mg per kg for lethality:
A toxic dose of 5 mg/kg body weight, a minimal lethal dose (MLD) of about 80 mg/kg are evaluated and compared with previous published data.
So already toxic and easily enough lethal, especially in older age.
Levomepromazine
Also spikes in April 2020.

Whilst not toxic by itself, it confirms ‘end of life’ pathways are what is being used to cause these spike in drugs. Every drug listed in an ‘end of life’ pathway in the UK spiked in April 2020, the same month there was a three-fold increase in the number of dementia deaths.
Same Month Media Outlets Reported A Spike In C19 Deaths
Bolton News gave this graphic:

The data fudging ONS claimed the majority of the deaths in April 2020 from COVID-19 was in care homes — the very same ones that ordered a spike in lethal doses of drugs:
And yet, in their absolute desperation to cover up this explosive story of the Mass Murdering of the Elderly, the media stuck their foot in it, and destroyed all credibility for their weak argument that old people — who were certified as dying from dementia, note, not COVID-19 — were being bumped off using End of Life drugs because COVID-19 is supposedly super-lethal…
Prime Minister Admits Elderly Not At Risk
…with this admission from the Prime Minister of the UK at the time, Boris Johnson:

MAtt as I read this chart an 80 yr old covid patient has a SIX per cent chance of dying and if you are under 35 your chances are negligible.
If I were an 80 year old and I was told that the choice was between destroying the economy and risking my exposure to a disease that I had a 94 per cent chance of surviving I know what I would prefer
You heard it directly from the Prime Minister himself. COVID-19 did not kill those elderly people.
Can We Prove It Even Further?
Yes! Above and beyond the call of duty! This was planned, before the pandemic.
That End of Life care home document showing lethal doses of Midazolam, is from… October 2012, before the pandemic even begun:

Midazolam appears again in end of life documentation from 2016 for the NHS:

MHRA didn’t give marketing authorisation for Midazolam until September 2020, months after April 2020, so the usage was entirely illegal (assisted murder isn’t legal in the UK anyway; unlicensed exactly like NHS Scotland says):

Metoclopramide hydrochloride — the injectable form of Metoclopramide — didn’t get authorisation until November 2021:

We knew none of it was moral. Turns out none of it was legal either! What’s the point in marketing authorisation if unauthorised drugs get used anyway?
What If They Were Just Stocking Up For An Emergency?
Emergency supplies are not permitted.
— CQC, on care home drug supplies
[…] We advise that care homes or individual patients should not routinely hold anticipatory medicines stock […]
— NHS notice, April 10th 2020
Out the window that bunk theory goes.
Medical Expert Weighs In
Our article, Mass Murdering Of The Elderly, prompted the weighing in of a medical expert: Prof Nursing Auditor Denise Gardiner, who gave us permission to republish their comment. People are encouraged to read the full original comment here, as we will be segmenting parts for the article.
Part of their comment, emphasis added:
Midazolam is rarely used outside of a surgical setting here in the USA. Speaking from years of experience as an independent prof nurse auditor, I have never seen this prescribed in any care-home setting in the US, I know it is sometimes used for people with poor clearance but it is rare. Lorazepam (Ativan) is the DOC anxiolytic prescribed here for the geriatric population so commonly prescribed for agitation/anxiety it is often referred to as Vit A among nursing staff. Oral tabs (po) are small, can be cut or crushed, and it is prescribed the majority of the time, rarely IM [intramuscularly] or IV [intravenuously] unless the patient can not swallow. Haloperidol is not prescribed often outside of the geri-psych population d/t SE, opioids are rarely prescribed for anything other than pain greater than 6/10 d/t high risk for constipation/impaction/blockage, delirium, CNS depression, drowsiness, and when they are prescribed it is a PRN and a bowel regimen must be in place, this is or was protocol. If I see opioids in the chart I'm looking for ALOT of documentation on pain assessment and a diagnosis of Cancer or other pathologies warranting their use.
Notice that injectables (IV — intravenous, IM — intramuscular) are rarely used according to Gardiner? Notice Midazolam is rarely prescribed outside of surgery (read: in a care home setting), which is why ICU experiences do not translate to care homes. Care homes are not a surgical setting.
Dementia is not cancer, so the odds of it needing or requiring painkillers is extremely low, especially not powerful drugs like Morphine, Diamorphine or Oxycodone.
Opioids (AKA Opiates) like Morphine are Schedule 2 in the UK, and require a controlled drugs cupboard and registry, requiring documentation, much like the US does. Ironically, Midazolam is Schedule 3, which means it doesn’t require storage in a drugs cupboard and need no paperwork.
A Forbes article, ironically about Midazolam’s usage in death penalty settings, confirms Midazolam is only typically found in surgical procedures:
[…] midazolam has no analgesic, or painkilling, activity on its own. In fact, the combination of midazolam, fentanyl, and propofol are used together for what's commonly called "conscious sedation," a type of incomplete anesthesia that works for short, outpatient surgical procedures or changing dressings for burn patients. […]
— Forbes, The Drugs Used In Execution By Lethal Injection
Surgeries are not a feature of care homes.
Increases Falls Risks
Denise continues:
All of the drugs listed in your article [ed: the Mass Murdering the Elderly article] increase Fall Risk which is serious, so if these drugs were prescribed, one or God forbid all four, then I'd be very concerned, enough so that patients records better have documentation, documentation, documentation.
As Gardiner notes, elderly patients are frail and at high risk of serious injury from falls. You can’t arbitrarily inject the elderly willy-nilly with sedative drugs just because it’s convenient. They become drowsy and can fall.
Ironically, NICE — the ones who issued the Midazolam advisory in April 2020 — warns about possible fall risks in the elderly.
Looks Like Assisted Suicide
After examining the evidence in the Mass Murdering Of The Elderly article, Denise concludes:
I'd think what the heck is going on here, and that I may have witnessed evidence of doctor assisted suicide.
The people given those drugs were murdered.
Indeed. And we’ve certainly made the case for it.
As mentioned in the words of Professor Patrick Pullicino:
Midazolam depresses respiration and it hastens death. It changes end-of-life care into euthanasia
But The Daily Beagle won’t stop, here are some eyewitness accounts to close the case.
Eyewitness Accounts
Screami Mimi remarked how they were unnecessarily offered anti-anxiety meds (similar to Midazolam) for what were breathing difficulties, which they declined and managed to survive their ‘double pneumonia’ experience:

Commenter David Lamb detailed their experiences of the system, some key excerpts:
I lost my father in a care home in December 2020, when the poison 'vaccine' first came out and they injected him without consent. He died three days later.
The injection without consent is damning by itself, with tragic consequences.
But for David the horror continued, where family had to fight to release his mother from hospital who was mysteriously getting worse:
After several days she was getting worse, and I knew something wasn't right. I was living in Pennsylvania, and talking to my sister in Arizona every day to stay in the loop with mom's condition. At this point I told my sister she has to go and just demand that they release our mom, and I told her I'll be on a plane within hours if they refuse. My sister went the next morning, and the doctors argued but did release our mother. She started recovering immediately upon getting home, and within a few days was fully recovered.
Recovering after leaving hospital? What were they doing to her?
They found out she was prescribed fentanyl… for kidney stones, only uncovered by a new doctor:
[…] the doctor says to her "why did they give you fentanyl when you were in the hospital for the kidney stone?"
Whilst fentanyl is used during surgery, it isn’t typically used in an outpatient setting given the smallest doses can be lethal. As it turns out, fentanyl is another alternative opioid used in death penalty injections.
The Daily Beagle Also Found Drug Crashes
We’re not entirely sure of the meaning, but we also found numerous drugs whose orderings crashed in April 2020 specifically. We note our findings here for posterity.
Anti-Inflammatories Crashed
It is interesting to note that anti-inflammatories would assist with COVID-19 symptoms. Notice five distinct types all crash
Adcortyl appears to be typically used in a care home setting to help with Rheumatoid Arthritis. We suspect similarly of the other drugs. When we queried the implications of the trend with the AI GPT-3, it pointed out that these drugs treat chronic conditions, which you wouldn’t need to keep ordering in if you knew the patient being treated wasn’t going to live long.
If they ordered in lethal dosages of drugs to bump off patients, it makes sense they would stop ordering in chronic drug treatments for said patients.
Cardiotoxic Analgesics Crashed
Cardiotoxic (heart poisonous) analgesics (painkillers).

Interestingly, Bupivacaine is listed on the assisted murder document. We do note however that Bupivacaine is also used by dentists, and dentists were forced to shut in April 2020, that said, they weren’t allowed to reopen until June 2020, which fails to explain why the drug purchasing crashed only in April 2020, and not also in May.
The toxic dose of bupivacaine is 2 mg/kg (with or without epinephrine). It is one of the more cardiotoxic local anaesthetics. Bupivacaine is therefore contraindicated for i.v. regional anaesthesia (IVRA) because of potential risk of tourniquet failure and systemic absorption of the drug.
The other drugs that crashed are listed as similars to Bupivaciane by their BNF (British National Formulary) codes (E.G. 1502010C0AAABAB), which all start with the first seven digits of 1502010. Notice how even over-the-counter topical (externally applied) creams and gels also drop, despite the fact pharmacies remained open during April 2020:
Lignospan Special 20mg/ml / 12.5micrograms/ml inj 1.8ml cart
Lignospan Special 20mg/ml / 12.5micrograms/ml inj 2.2ml cart
Topical creams are not typically used by dentists, although gels may be, they are also likely to be over-the-counter as well, and thus not exclusively the domain of dentists.
Whilst The Daily Beagle cannot prove it, we strongly suspect this to be a cover-up and/or data fudge, given entire categories (1502010 onwards BNF codes) of drugs — even ones that should have still been selling or used — seem to be zeroed out for just April 2020, the same month as the large spikes in assisted murder drug purchases.
Given the large quantities and variations of drugs, it seems to be a hamfisted attempt at squashing a massive data signal in a particular subset of drugs that appears to have squashed collateral, unrelated drugs. We cannot prove this, however we believe the evidence speaks for itself.
Even if we assume an innocent explanation for the squashed figures, none exists for the spikes in ordering for lethal dosages and subsequent administrations shown earlier.
The Elephant In The Room
One question to ask: was COVID-19 used as a cover story for killing off a large quantity of the elderly in care homes?
We have seen a sufficient quantity of evidence that has shown the purpose of these drugs is lethality, that their timing of their ordering, usage, overlaps with the timing of large quantities of deaths within care homes, despite there being no statistical justification for it, which you have seen admitted by the at-the-time UK Prime Minister himself, Boris Johnson.
It is doubtful The Daily Beagle, or anyone else, could compile a more compelling set of evidence for the case of the Mass Murdering of the Elderly in care homes, just short of the perpetrators confessing to the crimes outright themselves, which they are all but doing.
The question now becomes: what do we do about it?
Subscribe to receive more content like this from The Daily Beagle.
This is important.
Feel free to leave a comment below:
Hi Underdog / DB. Please see this BMJ study:
BMJ FMCH:
"Primary care.. Benzodiazepines, opioids.. Prescribing.. highest recorded.. coinciding with the UK peak number of deaths in April [2020]..
correlated strongly with total monthly deaths.."
Spearman’s rho Corr. ρ / April +%:
▪️ρ=0.93 / +78% Midazolam
▪️ρ=0.88 / +95% Levomepromazine
▪️(+30% +43% +60% Morphine tart.)
study:https://fmch.bmj.com/content/9/3/e001143
thread:https://mobile.twitter.com/JavRoJav/status/1625783114541805570
FB:https://www.facebook.com/rohail.javed.50/posts/pfbid033MW8RNqgpG96dvGQgqNov1c5mze1XJ8UGgmmMQKoAYoBpwmbTXmnHLSGU6SZFBwzl
(more in comments/below):
T:https://t.me/JavRoJav/236
Wow this is an amazing piece of work. I hadn't thought about the use of hyoscine + buscopan like drugs but of course it must have been terribly annoying for the people administering midazolam to have their peace interrupted by the death gargles of those being drowned in their own saliva, so they dried them out with more drugs.
I'd like to apologise for my cynicism but I don't think I should, knowing that this was a mostly treatable disease.
You know what doesn't treat COVID? Or any cold, or any post-viral pneumonia?
Haloperidol. Midazolam. Hyoscine. Diamorphine. Levomepromazine.
God forbid those crazy conspiracy theorists didn't have any influence on these doctors and care home managers. Otherwise they might have been given those dangerous hydroxychloroquine and azithromycin and zinc drugs. You know, the ones that killed nobody.