


Discussion: Hypothetical Treatment Modalities
It is time to talk novel ideas

Disclaimer: This is not medical advice, speak with a medical professional.

Lengthy Foreword and Warning

I’d like to take a moment to stress these treatment proposals — aimed at medical professionals and clinical researchers to investigate further — are not validated proposals. They are preliminary (early) research.
The Daily Beagle Is Not Omniscient
No matter how convincing the research presented here may be, there are hidden variables, unknown unknowns, where the treatment proposal is ill-suited, or may make an illness worse. It is impossible for me to know the specifics of individual patient cases. These are only presented as ‘hmm, interesting’ findings.
The Daily Beagle Is Not A Doctor

Please do not attempt to present me your individual medical cases, as the text-based Internet is an extremely poor medium to perform a diagnosis, and I will not attempt to diagnose or rationalise a treatment protocol.
Do Not Self-Treat

To stress how informal this is, I’m writing using the informal ‘I’ pronoun (rather than the usual professional writing standard of using ‘we’ under nosism), and have marked this as a discussion. I do not want people in panicked desperation rushing out to try to mock up an experimental procedure and accidentally hurting themselves in the process.
If you are a patient, you may present this to a medical professional currently treating your condition(s), however do not be surprised if they say no.
Do Not Blindly Follow What Is Written Here

If you are a medical professional and your patient has presented this article to you, I advise using your best judgment; whilst I have attempted to highlight risks and tried to select methodologies that minimise risks, I cannot know your patient(s) specific condition(s) and there may be unknown risks, so use caution. You may freely take any ideas presented here.

If you are a medical professional and you have objections, please feel free to raise them up in the comments section below. Please supply evidence of objections wherein possible so people may be able to evaluate your claims correctly.
If you are a non-medical professional, please do not present unevidenced treatment advice. Any unevidenced or dubious treatment advisories posted in the comments may be promptly deleted. Do not assume an undeleted post is valid (it may have been missed, or allowed to stand as part of a wider discussion or debate).
Yes, it might seem like I’m being a dick, but I am genuinely concerned about seeing people get hurt. I will be holding myself to the same standards; I will be quoting peer-review and studies where possible, plus I have put a disclaimer on my own work. No ‘just trust me bro’ here.
Needs Further Research

This is not written purely as a legal escape clause, I am genuinely concerned a misguided attempt at a treatment protocol (whether mine or others) on this article could result in harms. I simply wish to present findings for consideration by the medical community in the hopes it saves lives.
What I expect to happen is for the medical community to refine and test the treatment proposals written down here using their own first hand expertise, or object to it, referring to some evidence for why something can’t work.
Onto the proposals.
Treatment Proposal: Impeding Transfection And The Spread Of Cancer Cells With Ferric Ammonium Citrate
What is Ferric Ammonium Citrate?
Ferric Ammonium Citrate (FAC), which may also go by the name of Ammonium Ferric Citrate (AFC) and the compound (NH4)5[Fe(C6H4O7)2], but should not be confused with Ferric Citrate. Ferric Ammonium Citrate is soluable in water, Ferric Citrate is not, and chemically they are dissimilar (one contains ‘Ammonium’), so don’t confuse the two. Many search results will return just ‘Ferric Citrate’ incorrectly:

Solubility is crucial as it means it can travel around the bloodstream.
How can Ferric Ammonium Citrate (FAC) help prevent the spread of cancer?
FAC Impedes Transfection
In The Daily Beagle’s prior article, I discussed a possibility on how cancer could be spread faster in the article “Cancer Within Days”.

The shortstop summary from that article is that ctDNA (circulating tumour DNA) likely integrates into healthy cells, either via transfection due to LNPs (lipid nanoparticles) found in the shots, or during cellular division.
The amazing news is, Ferric Ammonium Citrate is reported to impede transfection, even in ovaries (although, caveat warning: only currently proven for Chinese hamsters)…


…the prevention in ovaries is even more amazing given The Daily Beagle’s concerns of transfection in the ovaries in the article “DNA Modifications Impact The Next Generation”.
This gives the first plausible weapon to fight back against transfection in general. There’s others, but we’ll come back to those later. It turns out…
FAC Impedes Cancer Spread
Obviously, the first mechanism one would suspect is if FAC impedes transfection, it would also impede ctDNA uptake into localised cells (A.K.A. transfection) and thus impede cancer spread.
In the preprint (read: not peer reviewed) paper “Iron Inhibits Glioblastoma Cell Migration and Polarization”, it discusses how there’s some sort of relationship between cellular iron content and how mobile glioblastoma (a type of cancer) is:

You might be a bit confused (‘where did this iron talk come from?’). FAC is used for Iron supplementation (caveat warning: there are different types of Iron supplements and they’re not typically FAC). In this experiment, they explicitly used FAC to impact the iron levels:

So there’s (unreviewed) evidence suggesting FAC does indeed impede the spread of certain cancers.
FAC Kills Certain Types Of Cancer
It also turns out FAC doesn’t just inhibit spread, it also kills certain cancer cells (but, warning, not all types of cancer). There are so many studies saying this that I am just going to rapid fire quotes (emphasis and comments in square brackets added):
It has previously been revealed that ferroptosis dramatically promotes the death of cancer cells and inhibits cancer cell proliferation, division, and invasion; however, whether AFC [Ammonium Ferric Citrate] induces ferroptosis has not yet been fully elucidated.
Ferroptosis — cell death by iron (basically).
[…] this study verifies that AFC [Ammonium Ferric Citrate] has the biological activity of activating oxidative stress injury in NSCLC [non-small-cell lung carcinoma] cell lines, leading to a decrease in their autophagy and inducing ferroptosis.
FAC does not treat all types of cancer (limitation warning):
Iron, presented as ferric ammonium citrate (FAC), dramatically inhibits cell survival in ovarian cancer cell types associated with Ras mutations, while it is without effect in immortalized normal ovarian surface epithelial (T80) and endometriotic epithelial cells (lacking Ras mutations).
— “Iron modulates cell survival in a Ras- and MAPK-dependent manner in ovarian cells”
FAC may need companion resources in order to work against certaint types of cancer:
K562 cells [lymphoblast cells isolated from the bone marrow of a 53-year-old chronic myelogenous leukemia patient] had significantly increased levels of ROS [Reactive Oxygen Species] production when exposed to LS081 [lead compound] in the presence of ferric ammonium citrate but not with iron or LS081 alone.
FAC with these companion resources can also potentially work against prostate cancer:
The proliferation of PC-3 cells, a prostate cancer cell line, was not inhibited by 10 μM ferric ammonium citrate or 10 μM LS081 when cultured in 10% FCS-RPMI1640 for 24 or 48 hrs (Table 1) or 72 hr (data not shown). However, as also shown in Table 1, treatment with 10 μM LS081 plus 10 μM ferric ammonium citrate for 24 hr or 48 hr significantly reduced the number of cells relative to controls.
Preprint non-peer reviewed paper suggests (potentially toxic?) ‘high doses’ (caveat warning: it does not say relative to what; this may only be in vitro, not in vivo) of FAC are needed to kill cancer cells. Also note it causes lipid peroxidation (this is likely how it impedes lipid nanoparticle transfection):
High-dose ferric ammonium citrate triggered cell death in all cell lines tested, increasing malondialdehyde levels, the by-product of lipid peroxidation and index of ferroptosis.
Further evidence FAC works for some cancers but not all (in my humble opinion: it may be it requires a companion component like LS081 or perhaps something else):
[...] we exposed FTC-133 and 8505C human cell lines to ferric ammonium citrate (FAC)-mediated iron overload, Erastin or RSL3 as ferroptosis modulators, to analyse intracellular mechanisms and relationship to CD71 levels. […]"
[…] Iron overload induces early responses in FTC-133 [thyroid cancer cell line, follicular] but not in 8505C [thyroid cancer cell line, anaplastic] cells […]
[…] Our evidence suggests that FTC-133 cell line, exposed to iron overload, reduced their viability and showed increased ferroptosis. […]
— “Anaplastic thyroid cancer cells reduce CD71 levels to increase iron overload tolerance”
FAC may not be suitable for use in people with age-related macular degeneration.
[…] Ferric ammonium citrate (FAC)-treated ARPE-19 cells and C57 mice were used to elucidated[sic] the mechanism of iron overload-induced RPE [retinal pigment epithelial] cell senescence. [cellular degradation] […]
[…] We found that iron level was increased during the senescence process. Ferritin, a major iron storage protein, is negatively correlated with intracellular iron levels and cell senescence. NCOA4, a cargo receptor for ferritinophagy, mediates degradation of ferritin and contributes to iron accumulation […]
FAC Inhibits Viruses
But wait, there’s more! It has been reported it inhibited viruses, even HIV (although note: not all viruses). Also note it is only FAC, and not variants of just iron or just citrates.
Here we found the iron salt ferric ammonium citrate (FAC) inhibited Influenza A virus, HIV virus, Zika virus, and Enterovirus 71 (EV71) infections. […]
[...] both iron ion and citrate ion were required for the antiviral capability of FAC, as other iron salts and citrates did not exhibit viral inhibition.
FAC’s Most Likely Treatment Modality
I am just spitballing here, so this isn’t medical advice, it is me speculating heavily on what I personally think the treatment modality may look like. It could be horribly wrong.
It is very likely any treatment involving Ferric Ammonium Citrate would need to be intravenously administered.

Whilst FAC exists as oral supplements, stomach acid will break down and destroy large portions of this, and entry into the bloodstream is regulated by the gut. Oral supplements may have inconsistent purity, and something like the grape juice effect can adversely impact dosages.
This may be a problem if you need to localise small amounts to a specific target site (read: delivering it straight into a tumour) in order to minimise potential (liver) toxicity and side effect, or if you need higher doses beyond what the gut can reasonably absorb.
FAC Questions
The real questions I cannot answer are:
Which cancers does it work on and not work on?
My list is limited but based on evidence I strongly suspect it does not work for all types of cancer (I suspect not all are vulnerable to the ferric pathway).
It is hard to tell if this is due to the lack of a ‘companion’ resource like LS081 or just due to the nature of the specific subtype of cancer.
Can it prevent all types of cancer spread, or only those that produce ctDNA?
What should the dosages be?
Targeted doses delivered into the tumour could likely be lower than general administration into the bloodstream
The upper ceiling for tolerance will depend upon the patient (liver status, age, size, weight, etc)
What should the strength per dosage be?
There’s a ratio of ferrite to citrates and ammonium that needs to be considered. Not all FAC is created equal and some have different percentages. 5% may not work, 20% might be too strong; or 20% might be too weak (to kill the cancer) but toxic for the patient. Hard to know with no data.
How frequently should it be administered?
Continuous with low dose, in bursts with high dose, continuously with high dose?
Any co-administrations?
Should a lead component (lead is known to be toxic to human health) like LS081 really be co-administered with FAC? Even if it kills cancer cells?
Are there any other chemicals or components that can work to enhance FAC’s effectiveness and lower total net dosages of FAC?
Are there any non-toxic analogues to LS081?
When should FAC be administered?
Early on, to inhibit cancer spread as early as possible? [Assumes: Low toxicity and safe.]
Mid-stage, as part of a broad-spectrum treatment modality? [Assumes: Mid toxicity and some risks.]
Late-stage, as a desperate last bid to save a patient after other treatment modalities have not worked? [Assumes: High risk toxicity with big risks.]
My Personal Opinion
In my humble, and totally ignorant, non-medical opinion: FAC should be a 20% strength early first line defence against cancer, administered initially as high dose bursts, and then continuously low dose (if it fails to clear initially but shows signs of improvement) as part of a broad spectrum cancer treatment protocol.
For HIV, I would say 40% strength early first line, using an aggressive, high risk strategy of high dose very frequently, in the hopes of gaining clearance during initial discovery, and tone down to low-mid dosage continuous if it fails to clear.
These figures are unscientific, ‘finger to the air’ numbers and would need to be revised based on toxicity and patient recovery feedback.
Dosage levels should be determined by the upper tolerance limits of the patient’s demographics and profile, using a ratio percentage of their upper dosage limit as the calculation baseline.
This is all purely speculation and should be corrected using real world results and not relied upon as a stringent treatment modality. I’m just giving my 2 cents.
Treatment Proposal(?): Impeding Transfection

This will be much shorter and more sparse than FAC, as there’s very little data out there, and when I tried to contact field specialists, none gave me a response. As a result, I had to fly blind on this subject domain.
Warning: these transfection inhibitors are toxic (arguably FAC is the only exception, being an over-the-counter supplement), and there’s very little data to back up these claims.
Anything that impedes transfection is going to interfere with normal body operations relating to DNA and generally is going to be toxic. So presume toxicity unless otherwise proven.
Cortisone
Readers of The Daily Beagle may recognise Cortisone as ‘that drug that got banned for use with SARS-COV-2’. Cortisone is an anti-inflammatory steroid (usually given by injection). Turns out, by ‘sheer coincidence’, it can inhibit transfection:
[...] when added before DNPs to the cells, cortisone can inhibit transfection by 50% (Figure 6d), probably due to the depletion of transport molecules, including nucleolin, GCR, and dynein, from the cytoplasm [...]
That was the only study I could find. No further comment.
Endotoxins?
Endotoxins are nasty stuff, so don’t go injecting it (hence the word ‘toxin’). Reportedly they can cling to the LNPs and interfere with them. I couldn’t find much data, literally only a product site mentions this off-hand.

[…] Endotoxins can inhibit transfection […]
— General Transfection, by addgene.com
Perhaps others can lend more credible sources of evidence for this?
Antibiotics, Polyanions?
Sourced from a patent (there is very little data out there on inhibiting transfections):

[…] In addition, several common components of cell-culture media, including serum, some antibiotics, and polyanions such as dextran sulfate or heparin, can inhibit transfection and/or cause cell death when cells are transfected in media containing these components. […]
— Patent US20130029418A1, Methods and products for transfection
The patent fails to identify which antibiotics impede transfection. I suspect any antibiotics capable of killing the antibiotics resistant bacteria carrying plasmids.
However, this is a very interesting coincidence, as per The Daily Beagle article “How To Make A Pandemic Worse...”. The article shows evidence of the intentional withholding and reduction in antibiotics prescriptions.

No further comment on antibiotics, just an interesting observation.
Dextran sulfate (brand name: Dextran) could/may be safe (no guarantees, seek medical advice!) for use given it appears to be a pre-existing drug. No idea on dosages required to fully inhibit transfection.
Interestingly, dextran sulfate is used to reduce the risk of thrombosis:

This and heparin (also mentioned by the patent) might sound vaguely familiar.
Heparin was mentioned in the the notice posted by the Intensive Care Society (ICS) — advisers of ICU in the NHS — back in April 2021, when they were discussing vaccine-induced thrombocytopenia and thrombosis (VITT). It was mentioned in The Daily Beagle article “Death By Dehydration In ICU”.
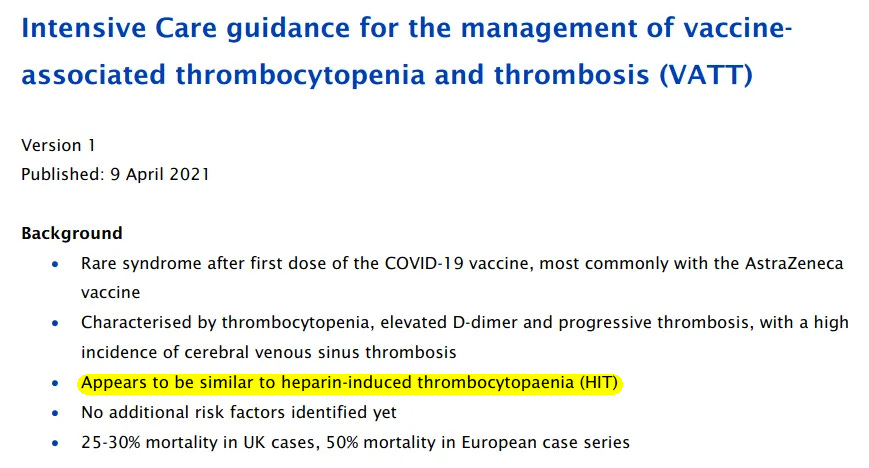
They remarked VITT looked similar to ‘heparin-induced thrombocytopaenia’ (HIT). Interesting coincidence.
FAC
As noted above, FAC also impedes transfection.
Treatment Modality?
Given the above (with the exception of FAC) are more toxic and can have adverse impacts, I am loathe to try to conjure up a speculative method of administering these to reduce transfections.
Nearly all of these cases (with the exception of FAC) are in vitro (put simply: done in a lab on a plate) rather than in vivo (read: used on a living thing).
For example, endotoxins are definitely toxic to humans, and are simply noted here for educational purposes. Perhaps their toxicity could be somehow neutralised but their ‘stickiness’ to LNPs could be retained? Or a new material using the same ‘stickiness’ developed?
No experts wanted to weigh in, and data was sparse. I apologise this isn’t the hard hitting journalism you had hoped for.
Treatment Proposal: Blood Filtration
I’m at the bottom of the barrel now, and the scraping noises can be heard. LNP toxicity in the blood is so novel that hard data on treatments simply does not exist, and trying to design ones when there are almost no LNP experts in the medical community is extremely difficult.
Queries Failed To Turn Up Results
I can state in total, I sent out queries to 6 of the most knowledgeable folks I have contact details for.
3 ignored my queries, 1 blocked me before I could ask (they also blocked a slew of other people). Only 2 people responded. 1 point blank declined to be quoted or named although we had a friendly discussion (I suspect they did not want to tar their fine reputation with something as lowly as The Daily Beagle). Of these respondents, only Jikkyleaks replied and said “magnetic filtration”.
As a result, I hope readers can forgive the very vague and very short proposals written here of possible blood filtration mechanisms. This presumes a sort of dialysis-style setup, but researchers/medical professionals, you can use whatever works for you.
Magnetic Filtration

The two words mentioned by Jikkyleaks are a semi-novel approach considered in blood filtration but hasn’t seen much traction.
It is unlikely it could remove LNPs unless they had a specific magnetisation, however, it might be possible to extract other blood components that do have magnetisation (read: separate some of the good stuff away from the bad; a reverse filter, of sorts).
It is impossible to know how successful this would be on reducing LNPs in the bloodstream.
Induce Lipid Peroxidation Via Phototherapy
Phototherapy is known to cause lipid peroxidation (read: destroys lipids). Obviously light cannot penetrate the skin, so the blood would need to be extracted, exposed and have the light proactively applied to it before it is put back in.

What’s particularly interesting is it causes ferroptosis-like deaths, much like FAC mentioned earlier. So it may also work on cancer cells by a similar mechanism. The above study also tells us what wavelength:
Tumors were then exposed to 660 nm laser light and the tumor volumes were monitored over 2 weeks (Fig. S24). PDT treatment significantly inhibited the tumor growth […]
660 nm would be a red light frequency. Not a fan of the number, personally.
The risks here is that the light could damage other blood components (good parts of your blood), and there’s no telling what that could do. Unknown unknowns. Needs further testing.
Some Sort Of Electrostatic Filtration
LNPs exhibit a Zeta Potential charge, which for simplicity sake means it is either positive or negative. It might be possible to isolate the blood from a patient and apply an electric field that ‘extracts’ or ‘isolates away’ the LNPs.
LNP Zeta Potential charge can also be changed by pH levels, so it may be possible to temporarily adjust the pH levels of the extracted blood to change the LNP’s Zeta Potential charge, and polarise it in such a way it can be filtered out by electrostatic attraction.
Alternatively, something like photoelectric application on the LNPs to cause their charge to change could make them dump their mRNA payload early — before they enter the cells — or possibly to aid in filtration.
I have no idea what this would look like, however (maybe blood pumped through a transparent tube with light applied to it, perhaps?).
Vibrations
One thing I learned from the EMA leaks is vibrations cause mRNA to degrade faster. Perhaps a machine that extracts blood, vibrates the absolute heck out of it, and returns it could destroy the payloads.
Or perhaps full body, with a high frequency vibration chair?
Clump ‘N’ Filter
Another idea is to separate parts of the blood from the patient, and during external blood filtration, intermix something like endotoxins or some other chemical that ‘clumps’ onto LNPs, and then use that to make it easier to filter the (relatively small) LNPs, then neutralise any remaining endotoxins post-filtration, before returning it.
Endotoxins are horribly toxic, hence the application outside the patient’s body, however ideally a better clumping agent would be used.
Centrifugal Filter
It may be possible to filter the LNPs by their weight, cutting off anything as light or lighter than LNPs. This might lose a few good blood components, but given the serious harms of the LNPs, may also help to remove the transfection reagents.
Are There Other Treatment Proposals?
There may be, however I struggle to keep up with the sheer amount of events ongoing (I am supposed to be a general news journalist). If people don’t want to share ideas on novel treatment modalities, I cannot force them to.
My own ability to devise new methods is limited by my lack of understanding of treatments and harms. But I must try, for the human race!
I’ve intentionally tried to avoid ‘obvious candidates’ people frequently mention online as I want to expand the discussion on possible treatments.
People I spoke with on Twitter seemed very browbeaten that the odds of this healthcare crisis seem insurmountable. I’m hoping this article proves this isn’t the case and that there’s always hope.
I’m hoping this also provokes a wider discussion on treatment modalities.
Stay sharp, dear reader.
Found this informative?
Help inform?
Thoughts, dear reader?
One type of blood filtration method has a name, and is available medically already:
plasmapheresis: "is a process of separating plasma from blood cells and replacing it with another solution. [This solution can either be synthetic or a donor plasma] It can be used to treat or prevent autoimmune disorders, infections, neuropathy and organ rejection."
Not medical advice, just noting it for educational purposes.
Endotoxin sticks to LNPs, Liposomes etc. altering Zeta Potential and thus Transfection.
My article from last August with links to more references.
https://geoffpain.substack.com/p/lnps-contaminated-with-endotoxin