
How Test Kits Are Used To Perpetuate COVID-19 Fraud
Perpetuated even to death certificates


Disclaimer: This does not constitute legal advice. Speak with a legal professional.
Correction: wrote ‘RT’ as ‘real time’ but it is ‘reverse transcription’.
Thanks to “Mr. F”, The Daily Beagle has received a collection of FOIA documents painstakingly gathered from various NHS hospitals indicating PCR (Polymerase Chain Reaction) Ct (Cycle threshold) values.

Before it is possible to grasp the serious ramifications, there has to be an understanding of how PCR tests work.
PCR Collection Kits
There are two parts to conducting a PCR test. The first part you may be intimately familiar with, collection, involving swabbing of an orifice on your body.

Swabbed material is then stored in a special preservative solution, which is sent to a lab to be used in an ‘analyser’ (American: analyzer) to determine a result.
The analyser portion is what we’re interested in.
PCR Analysis
Unsurprisingly, PCR works by ‘polymerase chain reaction’. But what does this mean?
Polymerase is an enzyme, and to oversimplify, something that interacts with things in your body. Very oversimplified: it causes genetic material to duplicate. You can repeat chain this duplication.
Literal descriptor: “a polymerase is an enzyme that synthesizes long chains of polymers or nucleic acids”; nucleic acid refers to things like RNA (ribonucleic acid) and DNA (deoxyribonucleic acid). The NA part, essentially.
Viruses contain RNA (such as coronaviruses), and some contain DNA (such as the genetically modified chimpanzee adenovirus used by AstraZeneca).
Supposedly, the PCR tests convert RNA to DNA, according to the ever unreliable FDA:

Synthesise means to fabricate, in the sense of ‘make more of’. Why would you want to make more? To make something easier to detect. Consider it akin to a magnifying glass that enlarges an image. Or a petri dish that breeds more bacteria.
But where does the polymerase get the energy to make more? And how long should you leave a polymerase to keep fabricating additional genetic pieces? How long is too long?
Enter The Cycle Threshold

The saw-see balancing act. The difference between positive or negative. A threshold determines where to stop; what’s stopped is the number of cycles. But what is a cycle? What does a cycle do?
According to ThermoFisher, one company that runs PCR analysis:
PCR steps of denaturation, annealing, and extension are repeated (or “cycled”) many times to amplify the target DNA.
One cycle consists of the following:
Denaturation (breaking down the DNA structure) using heat: “0.5–2 minutes at 94–98°C”
Annealing (binding of primers to the target DNA): “incubation time of 0.5–2 minutes”
Extension (extend the 3′ end of primers), which is where the synthesis of the so-called DNA “daughter strands” occurs
Essentially PCR uses heat to break down DNA structure, has primers bind to the broken down DNA, then has the primers ‘extend’ (make more of) the DNA, in a process that chains in a loop. Hence the words ‘chain reaction’.
Great. But how many times should we be doing this? Well, we need to set a threshold…
Where Should The Threshold Be?
What should the cycle threshold be? Well, ThermoFisher have this useful graph on their website:

Notice how on the graph it shows the results ‘plateau’ at 35 cycles onwards?
ThermoFisher remarks that (emphasis added):
[…] low cycle numbers are preferable for unbiased amplification (as in next-generation sequencing) and accurate replication of target DNA […]
They also remark (emphasis added):
The number of cycles is usually carried out 25–35 times […]
So, the lower the number of cycles, the more accurate it is, and less bias the amplification. We don’t want to do anything beyond 35 cycles according to ThermoFisher’s own graph.
What Do Governments Say On Threshold Cycles?
The UK government published their own graph which shows an element worse than ThermoFisher’s: it shows the plateau phase beginning at 30 cycles:

The RT stands for ‘reverse transcription’. The UK government identify the start of the ‘exponential phase’ at roughly 25 cycles. So between 25 to 30 cycles.
In the UK government document “Understanding cycle threshold (Ct) in SARS-CoV-2 RT-PCR” it notes several things:

Tests typically capped at a maximum of 40 cycles (suggesting there’s no real reason to go beyond this), and every 3 point increase in Ct (cycle threshold) value, a 10-fold decrease in the available genetic material required for it to register as ‘positive’. It would look something like this as an example:

So if we started with 10,000,000 (10 million) genetic samples inside a swab at 24 cycles, we’d only need 100 genetic samples at 39, and only 1 at 45 to test positive!
Even US government Anthony Fauci said the following lines in a video from microbe.tv:


[...] That if you get a cycle threshold of 35 or more, that the chances of it [the virus] being replication competent are miniscule [...]


[...] but you never, you almost never can culture a virus from a 37 threshold cycle [...]
Odds of a person testing positive with a PCR with a Ct of 35 or more being able to infect anyone is non-existent.
The implication of this statement is they don’t have the virus (if there’s no virus to infect others, then there’s none to infect themselves).
Translation: ~35 onwards PCR cycle thresholds are absurdly over-amplifying, producing bias results which unnaturally trend towards positive. False positives.
But Who Determines If It Positive?
Referring back to the UK government document “Understanding cycle threshold (Ct) in SARS-CoV-2 RT-PCR”, on page 7, they have an alarming set of claims:

In some cases they’re not told what the Ct values are (“Ct values are not provided”), so there’s no way to determine if results are worthless or not
Some systems that determine positivity don’t have any human oversight (“operator cannot observe the reaction”).
These software systems cannot be asked to show how it got to the conclusion the result was positive (“non-interrogatable”)
That is to say, some of the PCR tests are blackbox software that are literal walking ‘just trust us bro’ systems. Is the Ct value good? ‘Just trust us bro’. What does the reaction show? ‘Just trust us bro’. Were there any errors? ‘Just trust us bro’.
In other cases, we can infer a human operator must interpret the result, but that depends on the Cycle threshold. Which neatly returns us to the introduction of this article, with the question:
What Cycle Thresholds Did NHS Hospitals Use?
Determining if there is fabrication, we need to know the Cycle thresholds used in testing. “Mr. F”’s documents show the way, showing us what was used in NHS hospitals. Sarcastic remarks are in ‘inverted commas’.
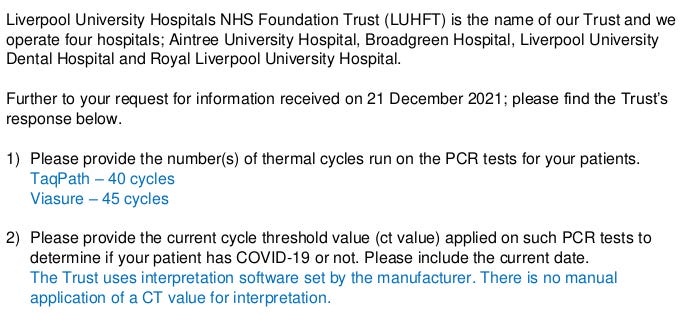
County Durham and Darlington NHS Foundation Trust: 40 and 45 Cycles.

West Hertfordshire Hospitals NHS Trust: 40 cycles (‘but the manufacturer made me do it’).

Liverpool University Hospitals NHS Foundation Trust: 40 and 45 cycles (‘but the manufacturer made us do it, trust me bro’).
Mid and South Essex NHS Foundation Trust: 40 and 45 cycles.

East Suffolk and North Essex NHS Foundation Trust (formerly 'Ipswich and Colchester Hospitals'): ‘hey bro some of our tests don’t have Ct values therefore we don’t need to tell you …’

‘… but here are the Ct values we don’t have’: >35 to >40 cycles.

University Hospitals Plymouth NHS Trust: 40 and 45 cycles.

The Princess Alexandra Hospital NHS Trust: ‘Wibbly-wobbly cycle threshold go brr’. Basically 45 (15 + 30 = 45), but also 34, and between 8 to 33 which are extreme ranges:

And The Refusals, Too
Every FOIA collection has to have the ‘special people’ who think they’re above the law.
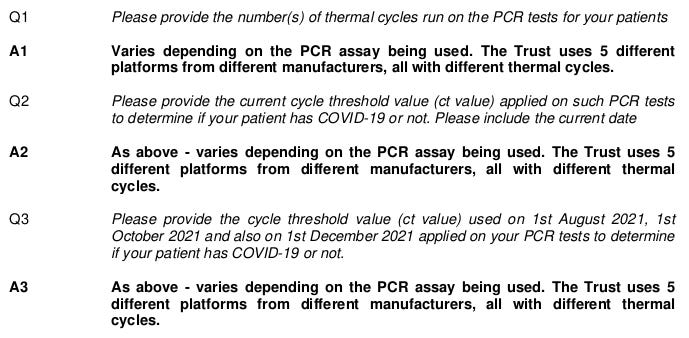
University Hospital Southampton NHS Foundation Trust: ‘well it could be one value or another depending on what test it is. We use 5 different tests. Counting is hard.’ A2 and A3 are literally copy-paste responses.
Northampton General Hospital NHS Trust (with ironic "dedicated to excellence" logo): ‘sorry bro we can’t tell you that or it would incite the public’. Also they added the highlighting themselves.

East and North Hertfordshire NHS Trust: ‘can’t tell you bro because our tests are speedy fast’. These are supposed to be medical specialists remember.

Manchester University NHS Foundation Trust: ‘we don’t need to tell you bro because someone else has a copy’. If they know where it is… they can just copy it in.

Stunning Conclusion: NHS Uses Rigged Ct Values
Fauci admits anything 35 or more is a worthless result. ThermoFisher, a PCR analysing firm, says values are usually between 25 to 35. UK government admits anything above 30 isn’t a useful result, anything above 40 is a typical limit.
What we have here are shocking admissions (or blatant avoidance) by major NHS Trusts using evidently rigged Cycle threshold values of 40 and 45. Way beyond any of this.
And It Gets Worse: COVID-19 Death Fraud Too
If you can accept anything beyond 34 Cycles are worthless false positives, then any declaration of death inferred from these over-amplified, bias results are fraudulent too.
Remember this quote? “A person who dies (for any reason) within 28 days of a positive PCR test”

It was the system initially introduced by Scotland during the early period of 2020:
The countries of the UK have been using slightly different methods. Scotland, for example, has only been counting deaths within 28 days of a positive test so that deaths from COVID-19 beyond 28 days are not included.
— Behind the headlines: Counting COVID-19 deaths, UK Health Security Agency
The UK government itself went far beyond this originally. It included anyone who tested positive and died regardless of date of test. Supposedly a “robust measure”. Emphasis added:
For several months, the COVID-19 Data Dashboard has been reporting, for England, all deaths in people who have a positive test. This a robust measure as it uses the fact of a positive test and the fact of death to derive the number reported. However, it is only an approximation of the number of people who die from COVID-19 because other causes of death are included and some people who die from COVID-19 never had a positive test. It was decided to adopt this measure in April in order to be sure not to underestimate the number of COVID-19 related deaths […]
— Behind the headlines: Counting COVID-19 deaths, UK Health Security Agency
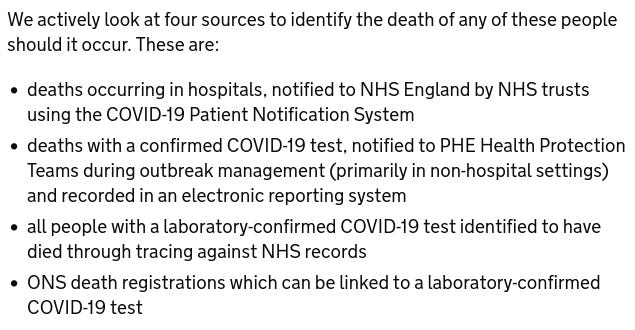
Wouldn’t want to underplay the fearmongering with accurate, well thought out statistics. How did they identify people were positive prior to death?
As the page notes, via NHS Trusts:
Uh oh! The same ones using broken Cycle threshold values. But surely someone, anyone, would have challenged the death certificate registraion, right?
Coroners Indemnified Against Challenge
How to stop people exposing the fraud? Prohibit examination!
The Daily Beagle was contacted by another person who wished to highlight the systemic fraud being perpetuated by the UK’s Coronavirus Act.
Within are excerpts granting coroners immunity to having their declarations of COVID-19 death findings being challenged, by suspending the requirement to hold an inquest, making the disease “non-notifable”:
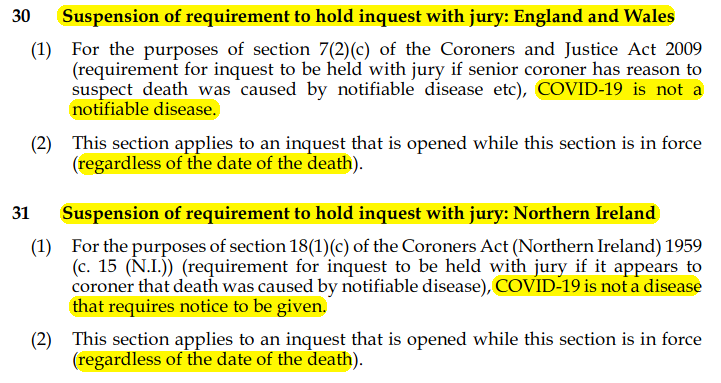
Non-notifable here means ‘nothing to note’ (rather than notification). As in ‘this classification isn’t at all surprising, totally normal, and you shouldn’t hold a jury inquest to investigate any further’.
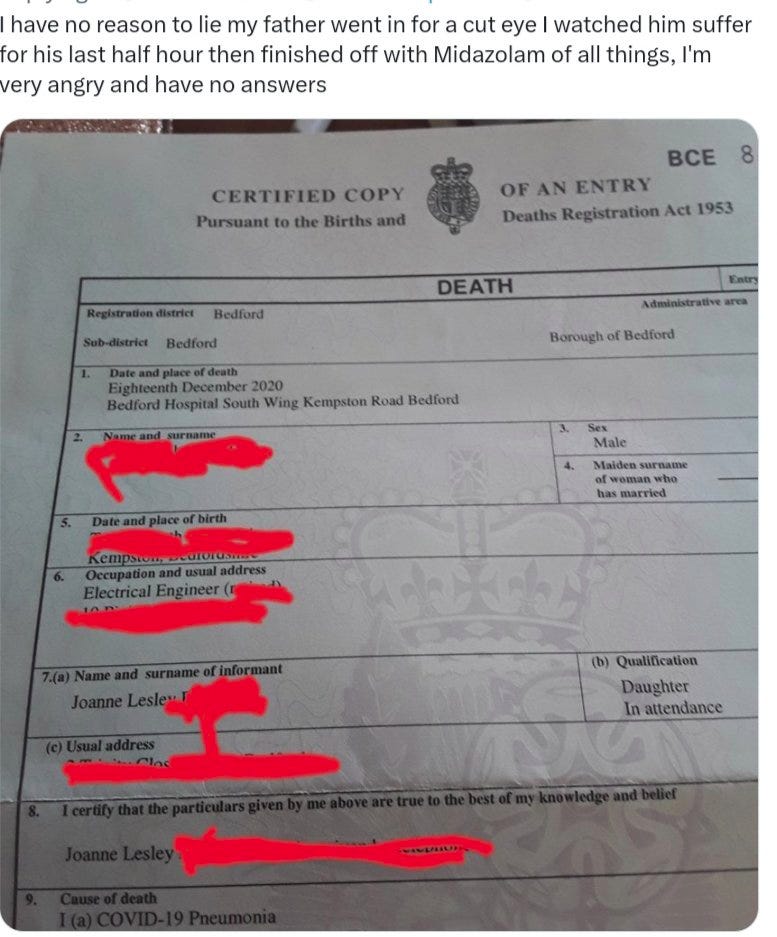
We have one example of a suspicious death on record, where one Twitter user posted how their family member was given Midazolam and died the same day…

…but was classified as being COVID-19 (bottom-left of the death certificate):
Wouldn’t Have Someone Noticed PCR Fraud Before?
In 1985 the PCR test was invented by Kary B Mullins, and it has been used — and criticised — in numerous crime cases prior to 2019.
The usual Cycle threshold? 28 cycles. Emphasis added:
[...] Polymerase Chain Reaction (“PCR”), a DNA testing laboratory will take samples of skin, blood, hair, and other DNA found at the scene of the crime and copy or “amplify” the sample’s nucleic acid sequence. This process is usually repeated twenty-eight times [...]
— By A Scintilla Of Evidence: The Issues Involved In The Admissibility Of Low Copy
That is to say, far lower than the rates the NHS Trusts were using.
[…] The risk of stochastic effects increases with the addition of extra amplification cycles […]
— By A Scintilla Of Evidence: The Issues Involved In The Admissibility Of Low Copy
Another term for ‘stochastic effect’ is chance effect. That is to say, random chance. So yes, PCR fraud has been noticed before. Amplifying a low quantity of DNA even has a name in legal circles: Low Copy Number (LCN):
When a DNA sample is found that is below 100 picograms, the amplification of the sample will be repeated for additional cycles to create a final sample large enough for analysis. The use of PCR on samples less than 100 picograms has been termed Low Copy Number (“LCN”) DNA testing.
— By A Scintilla Of Evidence: The Issues Involved In The Admissibility Of Low Copy
We won’t get into the weeds analysing the legal criticisms of Low Copy Number, as this article is extensive enough; the point is it is a known issue. Known by many courts, coroners, law enforcement members, acadamics, government officials. A known issue the public were not told.
But Aren’t The Other Tests Accurate?
It is worth noting that the line for deaths specifically states only PCR: “A person who dies (for any reason) within 28 days of a positive PCR test”.
This ought not to be confused with equally as common ‘Lateral Flow Test’ (LFT), also known as an ‘antibody testing kit’, which are those cheap plastic rectangular kits. Called ‘lateral flow’ because the tested liquid material flows laterally.

You can tell the difference between the two; LFTs you get the result at home, PCRs you send off to a lab before you get the result.
LFTs aren’t put into an analyser, and ergo, do not undergo thermal cycles, and are thus not subject to Ct values. But they are incredibly easy to spoof. So easy, even school children can do it. Using things like orange juice…

…and fizzy soft drinks (‘soda pop’ for Americans):

Essentially, anything acidic (such as fruit) will cause a Lateral Flow Test to render positive. That means if your saliva has any acidic food or drink in it, then you get a positive result.
This was confirmed by Alexander Edwards, researcher and developer of clinical and microbiological tests at the University of Reading School of Pharmacy in the UK.

Meanwhile, ‘fullfact’, on the other hand, like they did with the Midazolam murders, falsely denies this phenomena even exists:

Even though the mainstream BBC and Guardian accepts this phenomena exists. It is a straight-forward thing to test; buy an LFT, add some cola to it and watch the result. Just be aware some acids can be too acidic and can destroy the test lines instead.
Essentially, if a child can do it, a hospital inflating Cycle threshold numbers, government agency looking to bump up COVID-19 counts, easily can.
Remember: they required unvaccinated to get tested whilst they gave a free pass to the ‘vaccinated’. So these flubbed, bloated numbers are also being used to determine ‘vaccine efficacy’ and sell an even bigger lie, by skewering testing on unvaccinated to inflate numbers.
Conclusion: Garbage In, Garbage Out
Over-inflated Cycle threshold values. An overbroad definition of COVID-19 death for ‘any death with a positive test’. Midazolam murders classified as COVID-19. COVID-19 death certificates with no jury inquests. Tests beaten by school children. Cherry picked testing on unvaccinated to make vaccinated look favourable. After reading this, does anyone still trust the numbers?
Our future article will cover the serious implications — and harms — of treatment if you get classified as COVID-19 positive, and why this fraud is extremely harmful.
Subscribe to get more content from The Daily Beagle, and consider upgrading to paid to help support our work.
Vital? Share our work!
And leave a comment below:
Good post. But you appear to have missed the industrial scale PCR fraud being done in the UK lighthouse labs. There single gene positives were taken as diagnostic of covid, when 2 from 3 was the WHO and manufacturer standard. Up to 65% of positives at any one time were FALSE, and listed as such in ONS reports online.
https://www.bmj.com/content/372/bmj.n208/rr-3
Full paper: https://arxiv.org/abs/2102.11612
It is odd that we are all repeatedly shining the spotlight on PCR covid test fraud but not questioning in any way the use of PCR to detect flu. When covid came on the scene the multiplex kits were all updated to include flu and covid. Then flu disappeared. Odd that.
I'd like to see the cycle thresholds used in the US - State by State, hospital by hospital, clinc by clinic, lab by lab...