


Anti-Allergy Medication Goes Up With Vaccine Adverse Reactions
Corticosteroids also sharply dropped during the Midazolam Murders

Disclaimer: This does not constitute medical advice, speak with a medical professional.

I was invited by Substacker JP to respond to Geoffrey Pain’s request for prescribing data on adrenaline (American English: adrenalin) from any country, in relation to adverse reactions to the poison shots.

As I’m currently overwhelmed, I thought I ought to rush out a ‘quick’ response, but after writing, I realised it requires an in-depth clarification and discussion, especially given the ‘quick’ response was grossly oversimplified, bordering on being wrong and misleading, specifically, this line:
Anaphylaxis isn’t simply treated with just adrenaline.
Anaphylaxis is the extreme end of part of what you’d call an ‘allergic reaction’ spectrum. But, generally speaking, you do treat anaphylaxis with adrenaline, just it’s more complicated than it appears.
I was addressing Geoffrey Pain’s indirect reference to adverse reactions, of which allergic reactions are part, whilst trying to keep my response ‘short’ (easier said than done). In doing so, I foolishly swept up ‘allergic reactions’ and ‘anaphylaxis’ together. It is why I prefer writing articles.
They’re not the same thing, but they are part of the same spectrum.
Prevention Is Better Than The Cure
Anaphylaxis is the life-threatening condition (typically from an allergic reaction) that requires urgent intervention, and this is typically treated with an adrenaline shot.
Indeed, we do see EpiPen (brand name adrenaline shot made by Pfizer) go up in the prescribing database (ker-ching for murderous Pfizer):

However, there are contraindications (times when you shouldn’t use it), for example, ventricular fibrillation, cardiac dilatation, coronary insufficiency, organic brain disease (cough, prions) or atherosclerosis. Paramedics prefer to avoid using it if possible.
What I was trying to hamfistedly convey was typically anaphylaxis is prevented from occurring in the first place, as it’s typically the progressive development of an untreated allergic reaction. Yes, some are sudden, but not always.
During the early stages, allergic reactions are typically treated with anti-histamines (E.G. Fexofenadine Hydrochloride) and steroidal drugs (various corticosteroids). They’re generally speaking ‘safer’ and less impactful on your body.
Healthcare professionals are more willing to give these as a result. Early invention is better than late intervention in most cases. So most allergic reactions to the Pfizer shot will be “hidden” via the use of anti-allergy medications keeping them below the radar.
So what do we see?
Midazolam Murder Mysteries Returns
We see two interesting trends in the prescribing data. The first is during the March-April 2020 Midazolam Murders time window (for readers unfamiliar with the Midazolam Murders, see this article), corticosteroids — useful for treating lung inflammation in patients showing COVID-19 symptoms — fell like a brick:

I suppose if you’re trying to bump off the elderly, you have no use for life-saving corticosteroid drugs to reduce lung inflammation from COVID-19. Notice that the drug prescriptions have not recovered post-2021.
Current management strategies and guidelines published by NIH recommend the use of corticosteroids alone or in combination for moderate, severe and critical infected COVID-19 patients, who are hospitalized and require supplemental oxygen.
— “Corticosteroids for treatment of COVID-19: effect, evidence, expectation and extent”
Multiple randomized trials indicate that systemic corticosteroid therapy improves clinical outcomes and reduces mortality in hospitalized patients with COVID-19 who require supplemental oxygen
— “Corticosteroids”, NIH COVID-19 treatment guidelines
Anti-Histamines Skyrocket
Meanwhile, anti-allergy drug Fexofenadine Hydrochloride (one of the stronger anti-allergy medicines) spike following seasonal patterns, but noticably spike higher in June 2021 and June 2022, post poison shot rollout, with the average prescriptions overall increasing after 2020:

This is an ‘undersell’ as many anti-allergy drugs are over-the-counter, and thus won’t appear on the prescribing database radar (over-the-counter drugs do not require prescriptions), that is to say, this is a conservative, bare minimum estimate.
Notice there are hundreds of thousands of prescriptions versus a few thousand for adrenaline shots.
We also see another anti-histamine, promethazine hydrochloride, forming a cheese wedge take-off, going from 20k prescriptions to almost 40k:

We also see weaker anti-histamines like Cetirizine hydrochloride going down; it is worth noting Cetirizine is also available ‘over-the-counter’, so this could also be a trend of people not attending GP appointments and self-treating:

However, we also see anti-histamine prescribing data is seemingly ‘unchanged’; that is, net total of prescriptions hasn’t altered, explained by the fact weaker anti-histamines have been swapped for stronger ones, so the signal of worsening allergic reactions is obscured:

If we look at the category for “allergic emergencies”, we see the September 2020 and September 2021 spikes; we can also see in 2022 there’s this larger block between March 2022 and September 2022 (circled):

This is synonymous with adrenaline usage (chart is exactly the same):

Why Women?
Geoffrey Pain asked this question:
Why were 87.5% of Anaphylaxis cases Women?
Two key reasons are noticeable; survivorship bias and biodistribution. It’s time to delve into the world of why maintaining biological distinction and understanding is important.
Survivorship Bias
The classic example of survivorship bias is how, during WW2, Britain were trying to work out where the best place to put armour plating on a plane was.

They examined the bullet holes on the planes that had returned — the survivors — but failed to account for the planes that hadn’t returned. Their data was bias to the survivors of bad events, and hadn’t factored in the non-survivors.
After realising their error, they inverted it: the bullet holes were in areas a plane could survive; it was the areas they were absent where the fatal shots occurred: notice it includes critical areas such as the engines, the support for the tail, and the main sections for a wing.
Likewise, women are more likely to die from anaphylaxis, because they’re less likely to die from myocarditis, which impacts males:

In this case, it’s not possible for males to die from Anaphylaxis, if they instead end up dying from poison shot induced myocarditis. The Daily Beagle even presented evidence how PEG — a toxin found in the Pfizer shot — negatively impacts male mice.
Contrary to Hickam's dictum (‘a man can have as many illnesses as he damn well pleases’), a patient can only typically die from one thing (not counting revivals or Lazarus syndrome). So, if males are more likely to die from myocarditis, they’re not alive long enough to die from anaphylaxis, and vice versa for females.
Sexual Dimorphism (And Biodistribution)
Contrary to what you may have heard from your latest woke brigade politically correct police officer, humans are sexually dimorphic. This fancy term means males are physically distinct from females. If something ‘morphs’, it changes; ‘di’ is similar to ‘bi’ in it means ‘two’. So ‘two distinct changes’.
Why is this important? Typically women are shorter than men (blue line are males, black line are females):
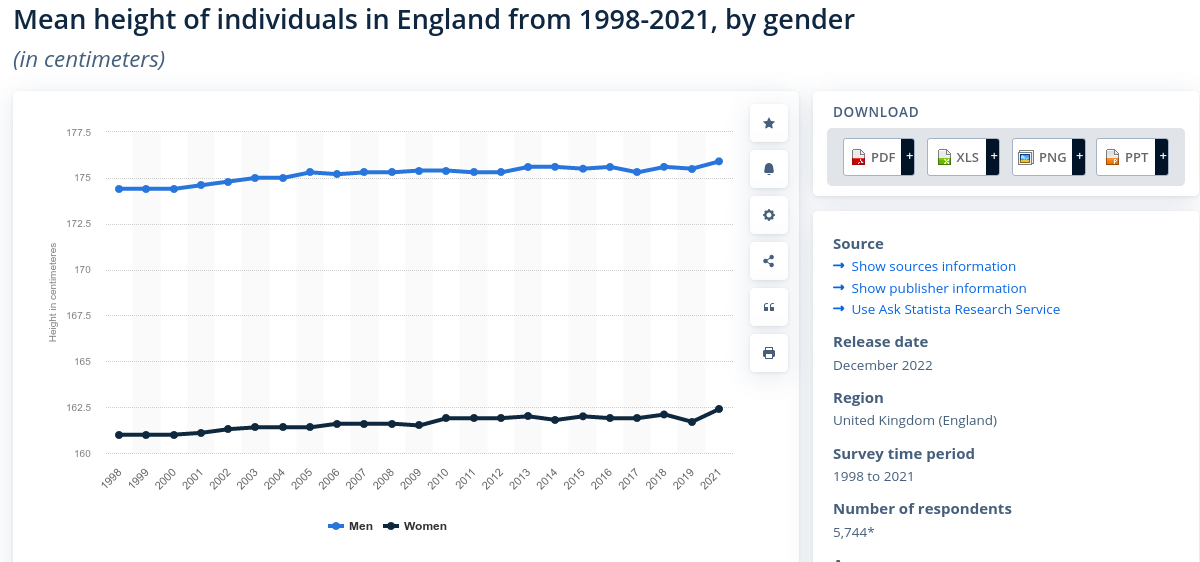
This means, females are typically smaller than males. Why is this relevant?
Those of you have undergone surgery requiring the use of drugs will likely know that a pre-op assessment includes taking your height and weight.
This is because the drug dosage you are given is proportionate to your size; essentially, it is how the drug will distribute (‘dilute’, shall we say) in your body.
Imagine it like adding flavouring to water: A small glass of water requires far less juice than a large bottle of water. Taller and bigger people require higher dosages than shorter and smaller people. It’s why children receive smaller portions of drugs.
So typically, women are given less drugs than men to account for their size. How does this apply to allergic reactions, well, we have to take into account…
Biodistribution
Males and females are given the exact same shot regardless of weight or size; I think any of you received a shot, will confidently assert not a single one of you got weighed or measured prior to receiving a shot.
You’ll be weighed and measured prior to receiving drugs, but not ‘vaccines’.
A ‘one-size-fits-all’ dose is reduced for children, but every child in a wildly varied age range will still receive that same dose, for example, the same dose will be given to a 6 month old and 4 year old despite the fact they are wildly different in development stages:

Pfizer admit there can be ‘dosing errors’ but their overly broad ranges essentially invite that to occur (imagine a 4 year old as big as a common 5 year old):

Notice there is absolutely no distinction for biological gender.
That means males and females get the exact same dosages. This is despite the fact females have smaller body sizes; and thus, the potent toxin is ‘less dilute’ in females, and therfore, far more toxic.
Per the EMA leaks, biodistribution of LNPs (lipid nanoparticles) and thus mRNA is a huge issue and unanswered question. One area it attacks is the liver, and other reports have gone over how it ends up in the ovaries.

This isn’t a complete response to Geoffrey Pain’s public query, but it should start the ball rolling.
Subscribe for free to the Daily Beagle to receive notifications of content.
Raise awareness!
And leave a comment below (public):
Would the Gremlins at Substack who undo settings I set, and insert typos I didn't write, take their booster shots, thanks.
Something to consider is many "anti-histamines" are anticholinergic too. I cannot take Benadryl. It makes me crazy. Imagine the myelin damage from the shots thrown in with a drug that blocks acetylcholine.
For a rush job, this was really effective. I never even considered dose dependency and that women would be more affected. The anaphylaxis corollary is damning. Your last piece disgusted me so much that I couldn't comment anything that wouldn't cause me grief. The secondary effects just continue to amass.
On a side note, I've started taking nattokinase after reading about spike shedding from the vaccines. My wife took the first round of shots and well I'm rather exposed to conditions from shedding. The whole Western population may be tainted to some extent from this "medicine."